
Dr. Ayesha Appa, a professor of medicine at the University of California, San Francisco, who treats addiction and HIV, prompted her medical student audience to envision a common scene: A man slumped on Geary Street, passed out from an overdose. How would students approach him?
With psychostimulant overdoses up 300 percent nationally from 2013 to 2019, the exercise is more realistic than hypothetical. Meanwhile, San Francisco is on track to have its deadliest overdose year ever in 2023, with some 692 deaths mostly due to opioids since October, and finding new medicines and practices to combat it is essential. But stimulants are also important to keep an eye on.
“Stimulant use disorder truly is a next frontier that will require all hands on deck,” Appa said during UCSF’s Grand Rounds on Thursday. What’s new and what’s working?
The “gold standard” to treat stimulant use disorder is simple positive reinforcement, called contingency management: For example, a patient who stopped using methamphetamines, evidenced by a urine sample, would earn a gift card. So far, evidence shows it works: Some 26 out of 27 studies measuring the efficacy of the approach for methamphetamines suggested a reduction in patients’ substance use.
“The idea is that, through operant conditioning and training a couple of times a week, someone is allowed freedom to make that change, and hopefully sustain,” Appa said.
About 92 percent of patients exposed to contingency management took their antibiotics to completion, and 87 percent had substance-free urine samples, Appa said. This year, a pilot program launched for contingency management but, for their part, San Francisco’s Veteran Affairs methadone clinics have used contingency management since 2011, and the health department has one.
What happens when a substance-use-disorder patient enters the hospital?
Dr. Marlene Martin, the director of the hospital’s addiction team, said she’s seen more and more patients hospitalized for substance use as the drug crisis worsens. As of 2018, one of nine patients were hospitalized nationally for substance use disorder.
One way to improve patients’ experience is by empowering primary care doctors to treat substance use, instead of relying solely on the addiction medicine team.
“When patients’ withdrawal is treated, you and they are comfortable; you see their true personality shine through,” Martin said. About two-thirds of patients who treat substance use in hospitals are motivated to use less, she said.
The UCSF addiction team specifically asks patients about substance-use history and health goals, and then tailors a health plan, such as prescribing medicines like buprenorphine or methadone, which are used to treat opioid substance use. But giving eye contact to a patient is as important as discussing their substance use. “This initial connection is so important,” Martin said, noting the “valid” distrust patients have toward medical institutions.
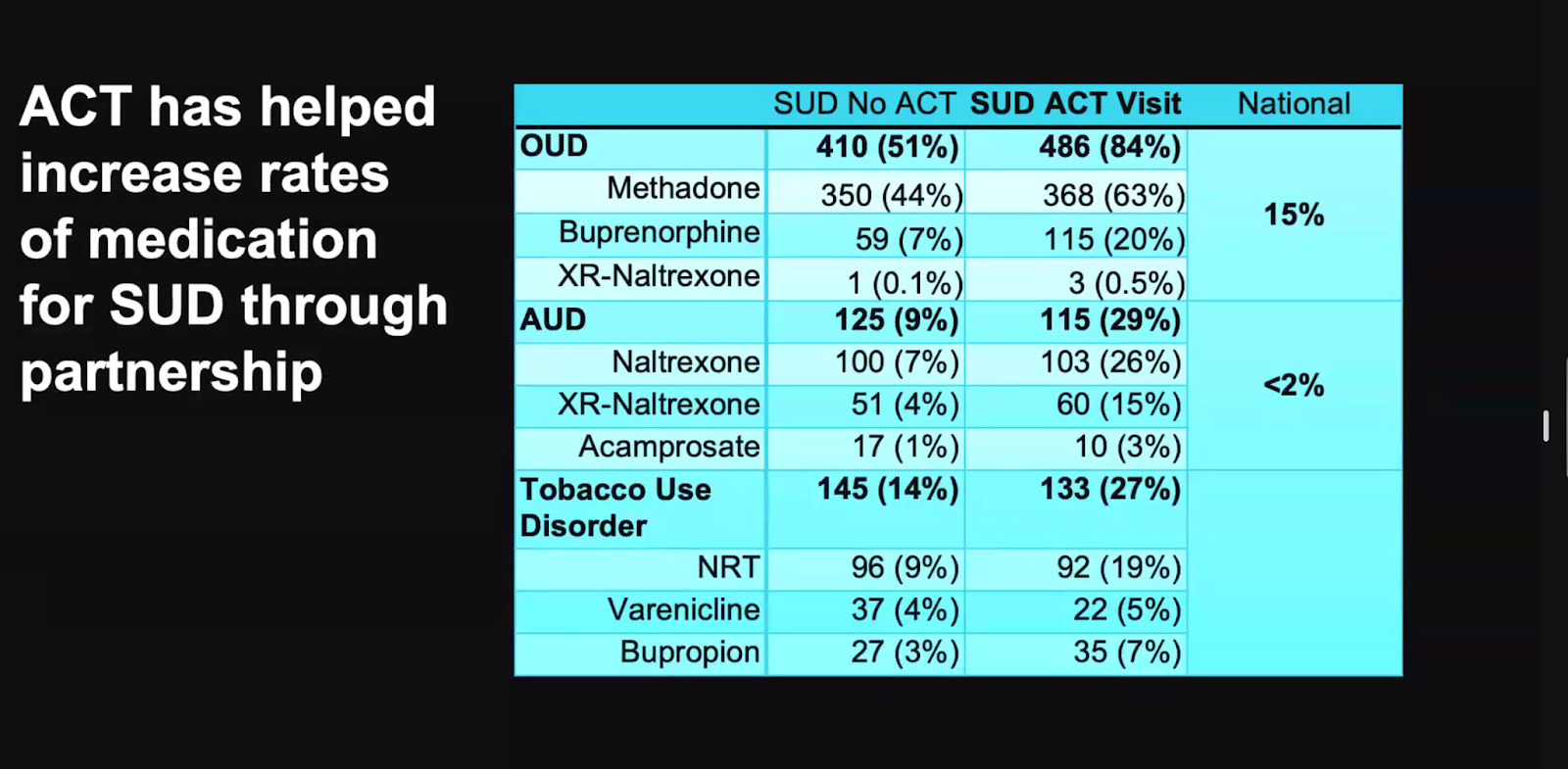
These practices appear to succeed. According to 2022 data, 84 percent of the addiction team’s patients started or continued taking substance use medicine, compared to 51 percent of those who did not engage with the team. Even the latter trumped the national hospital rate of 15 percent.
Looking forward, the hospital will train more board-certified nurses in substance addiction, and ramp up resources for those with alcohol use and liver disorder, alongside a substance-abuse educational program for Latinxs, called PEDAL, Program for Education in Drugs and Alcohol for Latine, that had its first meeting a few weeks ago, Martin said.
What happens when patients leave the hospital?
Christy Soran, the medical director of the Outpatient Buprenorphine Induction Clinic on Howard Street near 10th Street, said the key to keeping patients on opioid substance-use medicine is having “several doors” of care to walk through, and to offer low-barrier resources. Traditional medicines may not be preferred by the patient, for example, and sometimes severe withdrawal symptoms deter patients from taking drugs like buprenorphine frequently, Soran said.
Her team supports buprenorphine “overlap initiation,” which allows a patient to start on a lower dosage of buprenorphine than usually prescribed, but to take it more frequently; over days or weeks, the dosage is increased. Martin partners with pharmacies to administer the “complicated” doses. An evaluation of this method showed that more than half completed the overlap initiation, and “those who didn’t” returned a month later to try again. Of the overlap initiation participants, 10 to 20 percent had withdrawal symptoms.
Still, the results pleased Soran. “What that suggests to me is that it’s a low-barrier way for someone to try buprenorphine without having to wait for a period of withdrawal, and it was a good enough experience.”
Additionally, federal methadone distribution restrictions, which haven’t significantly changed in roughly 50 years, should be altered to ease access, Soran said. But she’s heartened that more clinics, both primary and specialty, are moving to incorporate addiction treatment and resources.
“We need to listen to communities most impacted by drug use, and people who use drugs to help solve this problem,” she said.


