Dr. Chinazo Cunningham, one of New York state’s leading experts on the opioid epidemic, has advice when it comes to treating addiction: Follow the data.
Addiction medicine is “so far behind” other medical disciplines when it comes to using data to guide treatment and identifying the most vulnerable, Cunningham suggested to a rapt audience Tuesday as part of the University of California, San Francisco’s Grand Rounds, a regular discussion on current medical news.
For example, data show that those most at risk of dying in an overdose are not the same people who use treatment centers most often, according to a recent data analysis of New York treatment centers done by Cunningham and her team at New York’s Office of Addiction Services and Supports, where Cunningham is commissioner. Nearly half the patients seeking addiction treatment in New York Office of Addiction Services and Support centers in 2022 were white, while a quarter were Black and 21 percent were Latinx.
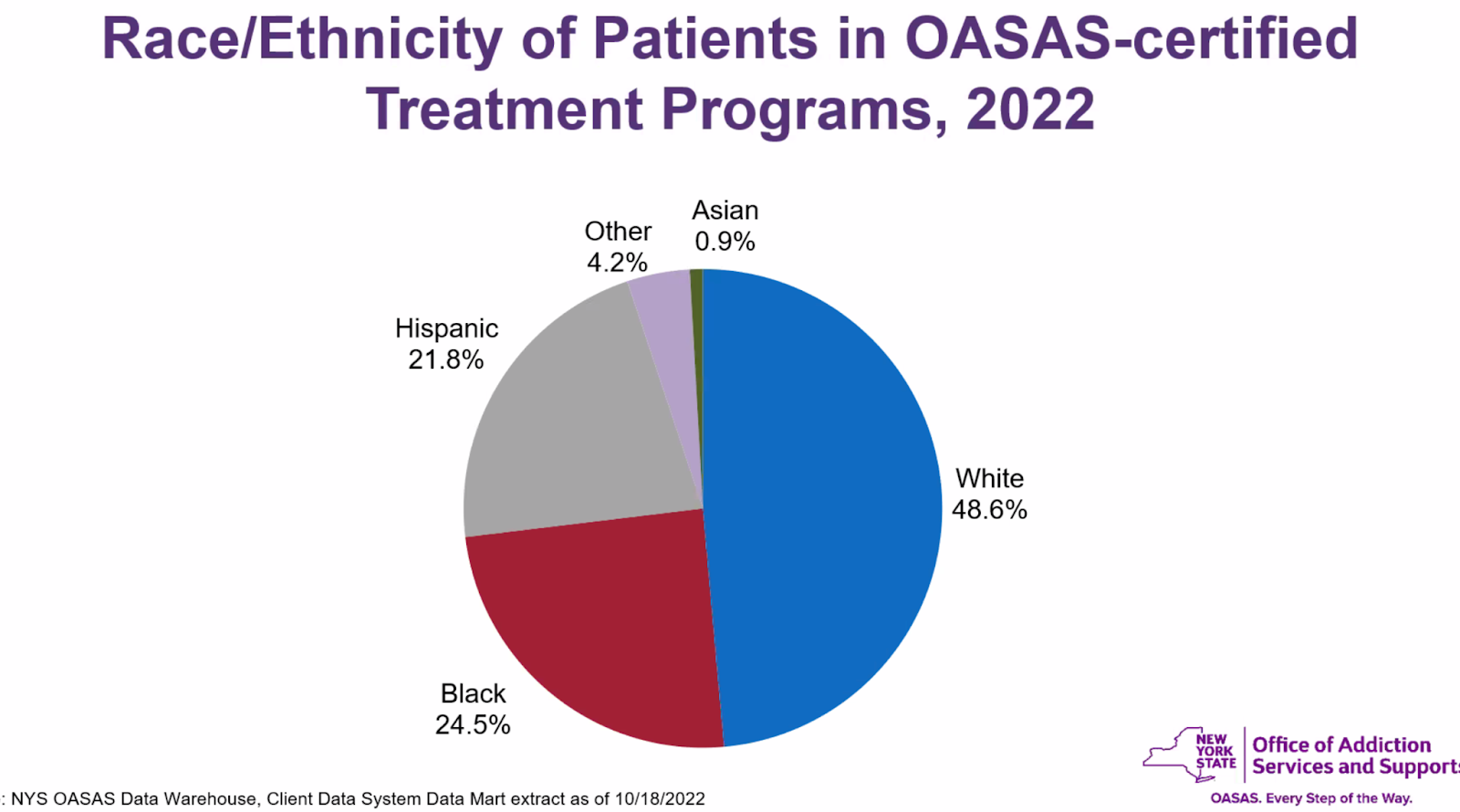
Black and Latinx residents, however, are far more likely to die from drug overdoses in New York state (and San Francisco) than white people, according to data analysis of deaths from 2018 to 2022.
“It doesn’t match,” Cunningham said.
Meanwhile, San Francisco reports some of the worst racial disparities when it comes to overdoses among Black residents. When Cunningham first saw the 2018 to 2022 data, in fact, she asked her team if they had committed an error. They hadn’t: Black San Franciscans are five times more likely to die from drug overdose than white residents, a disparity that is too absent from the public conversation, she believed.
Methadone vs. buprenorphine
Black and Latinx drug users may have to jump through more hoops when seeking withdrawal medication, Cunningham suggested. White people live in areas with more centers that prescribe buprenorphine, an opioid medicine that is more easily accessible, according to a 2021 New York-based study. Black and Latinx residents, however, had more access to methadone, an opioid medicine that is heavily regulated and sometimes harder to access.
“Why does this matter?” Cunningham rhetorically asked.
Generally, buprenorphine can be prescribed in higher doses, meaning a patient can get days of supply in one visit. Because methadone is more heavily restricted, patients who use it must register and visit a clinic daily, meaning visits sometimes happen “six days a week,” often early in the morning.
This, experts said, can mean skipped treatments, which is detrimental to a person’s recovery. Multiple medical experts note that the key to treating addiction requires “continuity” in treatment, which is why many advocate for 24/7 treatment centers and treatment in jails.
The fact that treatment availability is associated with race per the New York data suggests “this is a segregated system,” Cunningham said.
So collecting data should be regularly “evaluated” to ensure the best strategies are used, Cunningham said.
In Cunningham’s experience treating HIV-positive single-room-occupancy residents in the Bronx, she and her team thought most patients preferred to be treated in the SROs, so that’s where they often went. Instead, a study revealed they preferred to receive it most in the community-based drop-in center. Though “counterintuitive,” Cunningham used the information to change how her team treated her patients.
But it’s not just opioids. Stimulants like methamphetamine and cocaine were present in a sizable number of total fatal drug overdoses. In San Francisco, according to provisional data in 2022, cocaine was found in 42 percent of overdose drug deaths. Psychostimulants (excluding cocaine) were involved even more — some 49 percent — of San Francisco’s total drug overdose deaths. Indeed, a staff member at SoMaRise drug-sobering center told Mission Local in an earlier conversation that its clients were often taking meth.
But stimulants are hardly discussed in today’s conversations about addiction medicine, which centered on opioids and fentanyl. Cunningham found psychostimulants’ higher prevalence in California and San Francisco interesting, and implied that leaders should consider this data when looking at overall drug deaths.
California lags in offering safe-consumption sites
Cunningham pointed to promising initiatives elsewhere in the country: For the first time, New York state is requiring all jails to offer methadone, buprenorphine and another opioid-addiction medicine, naltrexone, to allow for the continuous treatment of the patient’s choice.
New York is easing access to buprenorphine and relaxing rules around methadone dosage, and the state’s Office of Addiction Services and Supports is increasing “mobile” units to prescribe medication to those who are hard to access. Rhode Island is piloting its first overdose prevention center — commonly known as a supervised-consumption site, where patients can take drugs under medical watch. New York City has two that have operated for almost two years. Centers are privately funded and not overseen by the state’s addiction agency.
But some places have not embraced these centers so readily. Gov. Gavin Newsom vetoed a bill that would have allowed a pilot of safe consumption sites in California. San Francisco toyed with opening its own, but declined, as it remains federally illegal to run supervised-consumption sites. (Cunningham didn’t opine on whether San Francisco should have one, specifically.)
The path forward, as Cunningham sees it, is to make mediation more desirable and get the best medical advancements into the hands of those who need it most.
Cunningham said, “advancements in healthcare are unequally distributed, and it’s our job to fight against that.”
It’s infinitely frustrating and depressing that so much money generated from so called “data-driven” tech companies in SF is funneled into supporting draconian tough on crime policies and candidates that conveniently ignore the data on addiction. Why is it that when it comes to drug policy all these VC ghouls (looking at you Garry Tan) and our dear Mayor just go on *vibes* and *feelings* rather than listening to the experts when it comes to drug policy?
That’s because whats been coming from New York “experts” was found in violation of the letter of the law as it stands today.
It should be obvious now that the fentanyl crisis is little more than a scare tactic, much like drug wars of the past. The real issues are police budgets and politicos’ platforms. The question for Breed and her whining tech mogul allies, addicted to power lunches and bank accounts, is not treatment, but eradication — not of the drug but the drug user. Why despite study after study, nothing changes? Because jail is cheaper and death is cheaper still. Yes, there are monsters roaming our streets with serious mental illness — too frightened to walk, so they ride in chauffeur driven limos, with dark tinted windows.
One reason why meth is not discussed in the same breath as opiates is that there are no effective treatments for meth addiction while there are, if rarely successful, for opiates.
Buprenorphine seems the best path forward, but the success of any opiate treatment is proportionate to the desire to clean up which is determined by the quality of life that an ex-addict is likely to face.
Drug punishers are the same ones who’ve supported neoliberal capitalism that’s traumatized almost everyone for the past 40 yr for fear of falling off of the edge after one misstep.
All overdose deaths in SF in which there is a positive test for fentanyl is “attributed” to fentanyl by DPH. Despite fentanyl’s lethality, it’s not an accurate portrayal.